

Donna D. Castellone, MS, MT(ASCP)SH
- Clinical Projects Manager, Hemostasis/Hematology
- Medical, Clinical, and Statistical Affairs
- Siemens Healthcare Diagnostics
- Tarrytown, New York
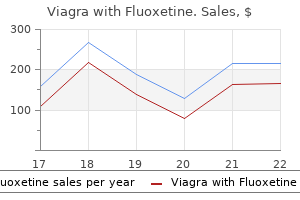
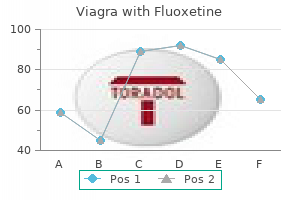
Growth factors can also be efficiently associated to synthetic or natural polymers impotence causes cures order viagra with fluoxetine. Such constructs induced differentiation of urine-derived stem cells into a myogenic lineage impotence treatments order viagra with fluoxetine discount, enhanced revascularization and innervation of the implants and stimulated in vivo resident cell growth [54] erectile dysfunction drugs used generic viagra with fluoxetine 100/60 mg line. Therefore buy erectile dysfunction drugs uk generic 100/60mg viagra with fluoxetine mastercard, the use of such models mainly aim to test the ability of decellularized tissues to promote (i) cell homing; (ii) regeneration of myofibers and motor neuron axons; and (iii) angiogenesis erectile dysfunction history buy 100/60mg viagra with fluoxetine amex. These are all essential steps necessary to have a functional skeletal muscle in the site of transplantation erectile dysfunction drugs free sample order viagra with fluoxetine on line amex. Moreover, acellular tissues have been used as natural devices in which host cells can drive muscle regeneration, as well as used as scaffolding material to deliver donor cells with the aim to improve cell therapy strategies. In order to evaluate the studies that have been reported so far, here we compare the results obtained among different acellular scaffolds and strategies- i. Although no details were reported in terms of functional activity of the implant, the authors concluded that the scaffold within the defect was associated with constructive tissue remodeling, including the formation of site-appropriate skeletal muscle tissue [26]. In this instance, Fisher and colleagues showed that the scaffolds promoted the formation of functional skeletal muscle cells, with perivascular stem cell mobilization and their accumulation within the site of injury [35]. Recently, few studies strongly supported the idea that decellularized muscles can offer a favorable environment to donor or host cells that promotes functional muscle regeneration [31,33,34]. Both innervation and in vivo force production were enhanced when implantation of bioconstructs was followed by an exercise regimen [31]. The table reports the studies in which decellularized tissues have been applied in vivo. The type of decellularized tissues, the method of decellularization, the type of the eventual seeded cells, the species subject to implantation, and the in vivo outcome have been reported for each reference. No functional recovery Skeletal muscle regeneration with partial functional recovery. Improved results for skeletal muscle scaffolds Skeletal muscle regeneration with partial functional recovery. No functional recovery Rat Improvement of donor cells survival Rat Partial skeletal muscle regeneration. No force restoration Rat Partial skeletal muscle regeneration Mouse Remodeling and partial skeletal muscle regeneration [22] [23] [24] [25] [26] [27] [28] [29] [30] [31] Rat Remodeling and partial skeletal muscle regeneration. The implanted construct promoted the formation of skeletal muscle and allowed the survival of donor cells nine months after surgery. Interestingly, a vesicular acetylcholine transporter was present on the surface of muscle fibers identified in the implant, suggesting the possible integration of the nervous system [22]. The decellularized muscle was prepared using an enzymatic protocol performed under agitation. Unfortunately, the aim of the study was focused on the immunomodulatory activity of the scaffold and muscle regeneration at the site of implantation was poorly characterized. However, the authors demonstrated that donor cells displayed better survival when delivered thought the scaffold, adding relevant information regarding the use of acellular matrix as scaffolding material for cell therapy approaches [24]. However, this functional improvement was associated with a concomitant reduction in graft-mediated regeneration, with coincident fibrous matrix deposition and interspersed islands of nascent muscle fibers. Such results indicate that acellular scaffolds can ameliorate the survival of delivered cells. The scaffolds were implanted in a model in which a portion of the lateral gastrocnemius had been removed. In this study, the muscular tissue was derived from dogs and decellularized muscles were obtained with an agitation method and an enzymatic and chemical decellularization process. Interestingly, the muscular scaffolds used in this particular study, prepared 308 Int. Altogether these results strongly support the idea that the protocol used to decellularize skeletal muscle is fundamental in determining if and to what extent the obtained scaffold is capable to improve the regenerative response of the hosting tissue. To address this point, some studies attempted to apply decellularized matrix to larger animal models. Even though the initial remodeling process followed a pattern similar to that reported in other studies, in the long term the implanted scaffolds showed dense collagenous tissue formation and islands of skeletal muscle with no successful restoration of tissue functionality [27]. Instead, a significant deposition of fibrotic tissue was observed within the defect region three months post-injury [30]. The authors reported that in all cases the acellular scaffold facilitated functional tissue remodeling, thanks to the recruitment of myogenic progenitor cells and improved innervation [32]. These clinical results are in contrast with those obtained from studies performed in large animal models [27,30]. More studies will be needed to determine if the reason for such discrepancies is related to species-specific biologic responses to decellularized scaffold implantation. Besides, it is also important to emphasis that so far muscular acellular scaffolds have not been tested in large animal models or patients. This conclusion seems to be valid not only when scaffolds are used as devices, but also when they are associated with cell therapy. The possibility of using decellularized scaffolds as devices represent an important aspect for their translational application, as it eliminates the limiting steps specifically related to cell therapy. Perfusion methods of decellularization appear to better preserve instructive cues necessary to promote functional muscle regeneration by host cells. The recently published method of composite tissue decellularization, strongly suggest the feasibility of applying such muscular scaffolds in large animals and patients [43,44]. Biomaterials based strategies for skeletal muscle tissue engineering: Existing technologies and future trends. Stem-cell-based, tissue engineered tracheal replacement in a child: A 2-year follow-up study. The role of extracellular matrix composition in structure and function of bioengineered skeletal muscle. Method for Decellularizing Skeletal Muscle without Detergents or Proteolytic Enzymes. An artificial niche preserves the quiescence of muscle stem cells and enhances their therapeutic efficacy. Basal lamina remodeling at the skeletal muscle stem cell niche mediates stem cell self-renewal. The pro-myogenic environment provided by whole organ scale acellular scaffolds from skeletal muscle. Myoblast-Acellular Skeletal Muscle Matrix Constructs Full-Thickness Abdominal Wall Defects. Functional Assessment of Skeletal Muscle Regeneration Utilizing Homologous Extracellular Matrix as Scaffolding. Co-delivery of a laminin-111 supplemented hyaluronic acid based hydrogel with minced muscle graft in the treatment of volumetric muscle loss injury. A Murine Model of Volumetric Muscle Loss and a Regenerative Medicine Approach for Tissue Replacement. Perfusion-decellularized skeletal muscle as a three-dimensional scaffold with a vascular network template. Bioengineered constructs combined with exercise enhance stem cell-mediated treatment of volumetric muscle loss. Decellularized muscle supports new muscle fibers and improves function following volumetric injury. Decellularised skeletal muscles allow functional muscle regeneration by promoting host cell migration. Codelivery of Infusion Decellularized Skeletal Muscle with Minced Muscle Autografts Improved Recovery from Volumetric Muscle Loss Injury in a Rat Model. An Acellular Biologic Scaffold Promotes Skeletal Muscle Formation in Mice and Humans with Volumetric Muscle Loss an Acellular Biologic Scaffold Promotes Skeletal Muscle Formation in Mice and Humans with Volumetric Muscle Loss. An acellular biologic scaffold treatment for volumetric muscle loss: Results of a 13-patient cohort study. Biocompatibility Evaluation of Tissue-Engineered Decellularized Scaffolds for Biomedical Application; Elsevier B. Perfusion decellularization of a human limb: A novel platform for composite tissue engineering and reconstructive surgery. Decellularized Human Skeletal Muscle as Biologic Scaffold for Reconstructive Surgery. Matrix scaffolding for stem cell guidance toward skeletal muscle tissue engineering. Skeletal muscle tissue engineering using isolated myoblasts on synthetic biodegradable polymers: Preliminary studies. Efficient delivery of human single fiber-derived muscle precursor cells via biocompatible scaffold. Functional muscle regeneration with combined delivery of angiogenesis and myogenesis factors. Skeletal myogenic differentiation of urine-derived stem cells and angiogenesis using microbeads loaded with growth factors. Restoration of Skeletal Muscle Defects with Adult Human Cells Delivered on Fibrin Microthreads. Tissue engineering of injectable muscle: Three-dimensional myoblast-fibrin injection in the syngeneic rat animal model. In vivo tissue engineering of functional skeletal muscle by freshly isolated satellite cells embedded in a photopolymerizable hydrogel. Protein-coated poly(L-lactic acid) fibers provide a substrate for differentiation of human skeletal muscle cells. The influence of electrospun aligned poly(-caprolactone)/ collagen nanofiber meshes on the formation of self-aligned skeletal muscle myotubes. Some of these unorthodox roles involve cell-cell interactions and are engaged to support immune functions such as leukocyte transmigration, recognition of opsonization factors, and stimulation of neutrophil extracellular traps. Other cell-cell interactions mediated by integrins include hematopoietic stem cell and tumor cell homing to target tissues. Integrins also serve as cell-surface receptors for various growth factors, hormones, and small molecules. Interestingly, integrins have also been exploited by a wide variety of organisms including viruses and bacteria to support infectious activities such as cellular adhesion and/or cellular internalization. Additionally, the disruption of integrin function through the use of soluble integrin ligands is a common strategy adopted by several parasites in order to inhibit blood clotting during hematophagy, or by venomous snakes to kill prey. Keywords: integrin; extracellular matrix; counterreceptor; disintegrin; immune system; stem cell; pathogen; virus; bacteria; venom; growth factor; hormone 1. Introduction the adhesion of cells to extracellular matrices is a fundamental requirement for multicellular organisms, and animals employ many mechanisms to fulfill this demand. Integrins are heterodimeric transmembrane proteins, made up of non-covalently paired and subunits, which serve as adhesion and signaling hubs at the cell surface. In mammals, there are 18 -integrin subunits and eight -integrin subunits that can combine to form as many as 24 unique heterodimeric receptor complexes [1]. Typically, ligand binding is carried out through integrin receptor recognition of small peptide sequences. Once bound to its ligand, an integrin not only provides adhesion, but also initiates signaling mechanisms which allow cells to respond to the mechanical and chemical properties of the cellular microenvironment. The inner ring depicts integrin heterodimers grouped into families based upon their classical binding profile. As a family of proteins, integrins and many of their downstream signaling intermediates have a long evolutionary history. Beginning at the root of the metazoan lineage, sponges have been shown to express - and -integrin subunits [3,4] that bind to peptides in a fashion similar to mammalian integrins [5]. Interestingly, integrin-encoding genes have been found in the single-celled eukaryotic 315 Int. This suggests that integrins and their aforementioned signaling machinery may have played an important role in the evolution of multicellularity. For example, integrins have been shown to interact with various proteins on the surfaces of eukaryotic, prokaryotic, and fungal cells, as well as a range of viruses. Within eukaryotes specifically, integrin-mediated cell-cell adhesion has been shown to coordinate a range of interactions and processes including leukocyte extravasation, stem cell homing, tumor cell migration, erythrocyte development, and interactions in the immune system. For infectious prokaryotes, integrins are exploited as cell surface adhesion receptors that mediate colonization and/or the bypassing of epithelial or endothelial barriers. Beyond mediating cellular interactions, integrins can also serve as cell surface receptors for hormones, growth factors, and polyphenols. Finally, integrins are also common targets for a class of small molecules called disintegrins, which are components of various snake venoms, and are also employed by hematophagous parasites. Integrin-Mediated Cell-Cell Interactions the first integrins discovered were isolated based on their ability to bind to fibronectin, which had itself just recently been identified (reviewed in [7]). However, in the early days of integrin research, several groups studying cell-cell adhesion in the immune system were also on the forefront of integrin identification (reviewed in [8,9]). In fact, integrins that mediate cell-cell adhesion in the immune system were among the first integrins to be characterized [8]. Nonetheless, it is important to understand that integrins are important mediators of cell-cell adhesion. The term counterreceptor has often been used to describe membrane-bound, non-matrix integrin ligands which facilitate cell-cell contact and will be used to differentiate them from the other non-matrix ligands in this review. Collectively, interactions between integrins and these counterreceptors mediate a range of immune cell functions including leukocyte extravasation from the blood stream, immunological surveillance in the gut, and hematopoietic stem cell homing and mobilization. All of these integrin-counterreceptor binding events serve to tightly adhere the leukocyte to the endothelium, enabling the white blood cell to cross the endothelial layer (a process known as transendothelial migration) in order to reach the inflamed tissue. Despite high homology between both integrins, they bind the iC3b fragment of complement via distinctive receptor sites, which may afford a greater diversity of leukocytes in opsonized target recognition modes [35]. This leads to the intriguing possibility of cooperativity between two integrins binding the same complement molecule [35]. Integrins act as "double agents" during Helicobacter pylori infection in the stomach, serving to potentiate bacterial pathogenicity while also aiding in the immune response.
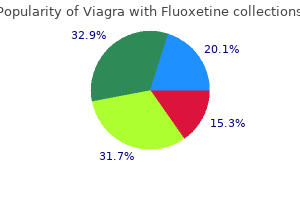
Its use up to 63 days (9 weeks) gestation remains offlabel but is widely established as a safe alternative to surgical termination of pregnancy venogenic erectile dysfunction treatment discount viagra with fluoxetine 100/60 mg fast delivery. Indication Medical abortion should be offered to all women seeking termination of pregnancy up to 7 weeks period of gestation (49 days from the first day of the last menstrual period in women with regular cycle of 28 days) erectile dysfunction pills generic order 100/60 mg viagra with fluoxetine overnight delivery. It is a safe method of termination of pregnancy so long the contraindications are not disregarded erectile dysfunction doctor san jose order viagra with fluoxetine 100/60 mg free shipping. The following information should be given to all those women who are suitable and who wish to have medical abortion: She will require visit to hospital/clinic on three occasions erectile dysfunction protocol food lists purchase viagra with fluoxetine mastercard. In case of heavy bleeding any time doctor who treats erectile dysfunction cheap viagra with fluoxetine 100/60 mg line, she will have to report to her doctor/clinic immediately to decide whether a suction evacuation is needed to control bleeding erectile dysfunction caused by high cholesterol purchase viagra with fluoxetine without a prescription. Her next menses may be delayed by one to two weeks, but subsequent menses will come on time. She has full option of choosing suction evacuation for terminating her pregnancy if she does not want to use medical abortion. During treatment and, preferably, till the next menses, she will have to avoid intercourse. She will have to sign a consent form after being satisfied with all the information provided, and after getting satisfactory answers to any doubts that she may have in mind. Dosage Schedule and Route of Administration She is instructed to take adequate rest and avoid going out of station. Third visit (day 15) A clinical history and pelvic examination should be done to ensure that there are no complications. Ultrasonography is required if history and examination do not confirm expulsion of products of conception. Standard dose for mifepristone is 200 mg given orally followed by 400 g misoprostol oral/vaginal according to the discretion of the clinician. Clinical protocol First visit (day 1) After a careful history, the woman is examined to confirm the uterine size, is counseled and an informed written consent is obtained. For vaginal use, misoprostol tablet should be moistened with a few drops of water and the women must lie in bed for half an hour. Misoprostol usually acts quickly and the women can expect to pass products of conception within the next few hours, but bleeding usually continues for several weeks She should be observed for 4 hours in the clinic/hospital. A pelvic examination is done before the woman leaves the clinic and if cervix is open and products are partially expelled, these are digitally removed. Patient should be advised to abstain from intercourse, or to use condoms, till the next visit. Surgical Termination of Pregnancy Indications Women seeking termination of pregnancy at a gestational age of 12 weeks or less. The alternative is medical termination with mifepristone/misoprostol if < 7 weeks Surgical abortion can be performed by aspiration (using an electric pump or a manual syringe) or by dilatation and evacuation (D&E) which is not a preferred method. Manual vacuum aspiration: Manual vacuum aspiration requires a single or double valve syringe: the vacuum (at least 55 mm Hg) is generated by a 60 mL handheld syringe which accommodates flexible plastic cannula ranging from 4 mm to at least 12 mm in diameter. Specific safety benefits of vacuum aspiration include a significantly reduced necessity of cervical dilatation, reduced risk of cervical injury, or uterine perforation, a reduced risk of infection and a reduced risk of blood loss, all resulting in a reduced need of anesthesia and a shortened hospital stay. The rates of major complications of conventional dilatation and evacuation/ curettage are two to three times higher than those of vacuum aspiration. Administer preoperative misoprostol for cervical preparation (400 microgram orally 3 hr before surgery). Cervical preparation reduces the need for mechanical cervical dilatation as well as reducing the risk of an incomplete evacuation c. Administer a single dose of oral antibiotic such as ampicillin 1 gm or a suitable alternative. Povidone Iodine or chlorhexadine solution to the pubic area, vulva, perineum and vagina. Insert sims speculum to expose cervix and clean cervix with povidone iodine solution. Vulsellum forceps or Allis tissue forceps are applied to the anterior lip of the cervix to control the position of the cervix. Dilate cervix with Hegar or Hawkin/ Ambler dilators starting with smallest dilator to a size appropriate for gestation. As a general rule, the dilator size will be equivalent to the number of weeks of gestation). Then, apply suction and move the cannulae with a circular motion while slowly withdrawing it until the uterus is empty. When the uterus is empty, a strong uterine contraction can be felt as the uterus grips the cannula, making the aspiration more difficult. Hypertonic saline: Taking aseptic precautions, a spinal needle is passed through the abdominal wall into the amniotic cavity. A variable amount of the amniotic fluid surrounding the fetus is removed and Table 36. Effectiveness: 81% will abort by 48 hours, with a mean time to abortion of 30 hours. Complications: Significant complications includes hemorrhage, clinical coagulopathy including disseminated intravascular coagulopathy, hypernatremia, renal failure and cervical laceration. When an inadvertent intravascular injection occurs, urea rapidly traverses cell membranes and acts as an osmotic diuretic. Dose: Intraamniotic instillation of 40% urea solution (80 gm of urea in 200 ml of distilled water) is used with intravenous oxytocin drip. Intra-amniotic prostaglandins: Instillation of prostaglandin inside the amniotic fluid acts as a reservoir, slowly allowing the prostaglandin to cross the sac to stimulate the myometrium. Side effects: Vomiting, hemorrhage, genital injury including cervical laceration, infection and retained placenta. Ethacridine lactate: Ethacridine lactate is a yellow dye with antiseptic properties. It is thought to stimulate endogenous prostaglandin production and subsequent uterine contractions. A no 16 Foley catheter is passed through external os for about 10 cm from internal os between the membranes and deciduas and the balloon is inflated with 30 ml water. Intravenous oxytocin is often administered concomitantly to expedite fetal expulsion. Effectiveness: the abortion rate is 45% at 24 hours, 72% at 48 hours, and 93% at 72 hours. Intravenous Oxytocin In order to further improve efficacy of second trimester inductions and to decrease the induction to abortion interval, combinations of intrauterine agents have been investigated such as hypertonic saline plus prostaglandin F2 and urea plus prostaglandin F2. This preparation has the advantage of being stable at room temperature and inexpensive. However, sublingual and buccal misoprostol have also been widely used, as they are more convenient to administer and may be preferred by patients. Dosage: Studies suggest that the ideal dose of vaginal misoprostol for second trimester induction is between 200 and 600 g and the ideal dosing interval is between 3 and 12 hours. Mifepristone in Combination with Prostaglandin Analogue Surgical Methods the most dramatic improvement in second trimester induction abortion technology has come with the introduction of mifepristone. The induction to abortion interval has been dramatically reduced when mifepristone is used before prostaglandin analogues. It is highly safe and effective (97% success rate) method and adverse effects are similar to that of misoprostol only regimens. Dilatation and evacuation: Dilatation and evacuation (D&E) is the standard method at gestations above 13 weeks in many parts of the world but infrequently practised in India. It is the safest and most effective surgical technique, where skilled, experienced providers are available. Depending on the duration of pregnancy, preparation to achieve adequate cervical dilatation can require from 2 hours to 2 days. Hysterotomy: Hysterotomy is an operative procedure in which the products of conception is removed before viability by making an incision on anterior uterine wall Hysterotomy has limited role in present abortion practice since its morbidity is markedly higher than medical methods. However, at times hysterotomy may be considered such as: (i) Failed second trimester medical induction, (ii) Presence of uterine anomaly (iii) Scarred uterus and woman is willing for tubectomy. Complications: Peroperative bleeding, anesthetic hazards, abdominal wound infection, scar endometriosis, scar rupture in future pregnancy. Women with clinical signs of failed abortion should be offered a uterine evacuation procedure as early as possible. Incomplete abortion: Incomplete abortion is also more common following medical abortion than following vacuum aspiration when the abortion is performed by a skilled provider. Vacuum aspiration is recommended over D&C for uterine evacuation, as it is associated with less blood loss, less pain and shorter procedure times. The recommended misoprostol dose and route of administration for this indication is either 600 g oral or 400 g sublingual. Hemorrhage: Hemorrhage can result from retained products of conception, trauma or damage to the cervix, coagulopathy or, rarely, uterine perforation. Depending on the cause of the hemorrhage, appropriate treatment may include re-evacuation of the uterus and administration of uterotonic drugs to stop the bleeding, intravenous fluid replacement, and, in severe cases, blood transfusion, replacement of clotting factors, laparoscopy or exploratory laparotomy. Common signs and symptoms of infection include fever or chills, foul smelling vaginal or cervical discharge, abdominal or pelvic pain, prolonged vaginal bleeding or spotting, uterine tenderness, and/or an elevated white blood cell count. When infection is diagnosed, administer antibiotics and, if retained products of conception are a likely cause of the infection, re-evacuate the uterus. Uterine perforation: Uterine perforation during the performance of suction evacuation or dilatation evacuation is a potentially serious complication that can result in hemorrhage or visceral injury. Perforation commonly occur during introduction of uterine sound or dilator and common site of perforations is the junction of the cervix and the lower uterine segment Perforation can be suspected when there is sudden loss of resistance with free mobility of the instrument, no tissue is obtained, when instruments are inserted deeper than expected, or when obviously maternal tissues such as omentum are obtained. When the uterus is already empty before a perforation is first suspected and the perforation is thought to be midline, then intraperitoneal bleeding is unlikely. If the pain and bleeding continue to be minimal, repeated pelvic examinations are negative, and vital signs and repeat hematocrit are stable, antibiotic treatment and observation for several hours are all that is necessary. Under any other circumstance, she should be admitted to a hospital for observation and possible laparoscopy or laparotomy. If the laparoscopy examination and/or the status of the patient give rise to any suspicion of damage to the bowel, blood vessels or other structures, a laparotomy to repair the damaged structures may be needed. If the abortion is not complete at the time perforation is suspected, abortion should be completed with the aid of laparoscopy. Uterine rupture: Uterine rupture is a rare but catastrophic complication that can result in hysterectomy. It is associated with later gestational ages and uterine scar, but has also been reported in women without these risk factors. Anesthesia related complications: Local anesthesia is safer than general anesthesia, both for vacuum aspiration in the first 380 Essentials in Gynecology trimester and for D&E in the second trimester. Write short notes on mm Hg pressure is generated in manual vacuum aspiration by a ml hand held syringe. Clinical guideline South Australian perinatal practice guideline First trimester medical and surgical termination of pregnancy Nov 2013. Comprehensive abortion care Training and service delivery guidelines Ministry of Health and Family Welfare Government of India. International Planned Parenthood Federation First trimester abortion guidelines and protocols Surgical and medical procedures. To differentiate between a cystocele and Gartner duct cyst-in cystocele catheter tip can be felt below the bulge. Uterine curette is used for scraping of the endometrial cavity to obtain sample for histopathology or therapeutic purpose during dilatation and curettage operation (D&C) or dilatation and evacuation operation (D & E). Sometimes to hold anterior lip of cervix in Nulliparous women during D&C operation. It can also be used to inject methylene blue dye into endometrial cavity during laparoscopic chromopertubation. In hydrotubation medicated solution (dexamethasone 4 mg and 80 mg gentamycin in 10 ml normal saline) is instilled transcervically in conditions such as following tuboplasty operation. Usually the anterior lip of the Uses For holding sponge or gauge piece during antiseptic dressing in abdominal and vaginal operations To hold polyp during polypectomy operation Instruments, Specimens and X-rays 385 To catch a bleeding vessel deep into the pelvis. During gynecological minor procedures like taking Pap smear, insertion and removal of Cu T, colposcopy, taking swabs. The other end is used for collection of vaginal cells from fornices for the hormonal status. Instruments, Specimens and X-rays 387 Can be used for taking cervical and vaginal smear for cytology and bacteriology. Uses In D&C operation-It is used to confirm position of uterus, to measure length of uterocervical canal and acts as first dilator. To empty the bladder in retention of urine To administer oxygen As tourniquet during myomectomy operation. For introduction of normal saline inside uterine cavity during sonosalpingography. Sponge holding forceps has catch but ovum forceps has no catch to minimise trauma if accidentally uterine wall is grasped Uterus is identified by: Pear shaped Attachments of fallopian tubes and ovaries Presence of cervix identified by external os. In nulliparous women external os is circular and in parous women external os is transverse slit like.
Cheap 100/60mg viagra with fluoxetine otc. Best 5 Natural Remedies for Erectile Dysfunction.
It is associated with either central or peripheral reduction in vision and not surprisingly is most common in the elderly drugs for erectile dysfunction list buy generic viagra with fluoxetine pills, although it can occur in younger people also impotence yahoo order viagra with fluoxetine canada. The images may be static or in motion erectile dysfunction treatment new orleans discount generic viagra with fluoxetine canada, and the importance of this diagnosis is as a distinction from psychopathological causes of hallucinations erectile dysfunction treatment melbourne buy genuine viagra with fluoxetine online. Peripheral lesions of sense organs may play a part in hallucinations in organic states erectile dysfunction morning wood buy viagra with fluoxetine 100/60mg on-line, and it has been shown that negative scotomata are to be found in patients with alcohol misuse erectile dysfunction treatment boots purchase viagra with fluoxetine on line. It has been suggested that the sensory isolation produced by deafness may cause paranoid disorders in the deaf (Cooper, 1976). Similarly, sensory deprivation due to the use of protective patches may contribute to the delirium that follows cataract surgery, along with mild cognitive deficits due to ageing. She was reassured by a psychiatrist, who saw her before and immediately afterwards, and promised to see her whenever requested during the post-operative period. Disorders of the Central Nervous System Lesions of the diencephalons and the cortex can produce hallucinations that are usually visual but can be auditory. Hypnagogic and hypnopompic hallucinations are special kinds of organic hallucination (see below). Hallucinations of Individual Senses Before deciding that a patient is hallucinating, the possibility of other explanations must be considered; these are not necessarily of pathological significance. The differential diagnosis of hallucinations includes illusions, pseudo-hallucinations, hypnagogic and hypnopompic images, vivid imagery and normal perceptions. Auditory hallucinations may be elementary and unformed, and experienced as simple noises, bells, undifferentiated whispers or voices. Elementary auditory hallucinations can occur in organic states and noises, partly organised as music or completely organised as hallucinatory voices, in schizophrenia. As well as occurring in organic states, such as delirium or dementia, they can occasionally occur in severe depression, but they are usually less well formed than those described in schizophrenia. Hallucinatory voices vary in quality, ranging from those that are quite clear and can be ascribed to specific individuals to those that are vague and which the patient cannot describe with any clarity. Patients are often undisturbed by their inability to describe the direction from which the voices come or the sex of the person speaking. A number of patients (becoming fewer in number with advances in treatment) have continuous hallucinations that do not trouble them. For others the persistence of the hallucinations cuts across all activities so that the patient is seen to be listening and even replying to them at times. The patient may also complain that their thoughts are no longer private but are accessible to others. This is known as thought broadcasting or thought diffusion (also a first-rank symptom) and is best classified as a disorder of thought rather than a hallucinatory experience, since there is no necessary implication that thoughts must first be heard. They may insist that the voices are the result of witchcraft, telepathy, radio, television and so on. Sometimes they claim that the voices come from within their bodies such as their arms, legs, stomach, etc. For example, one patient heard the voices of two nurses and the Crown Prince of Germany coming from her chest. Some patients hallucinate speech movements and hear speech that comes from their own throat but has no connection with their thinking. However, it has been shown that sub-vocal speech movements occur in healthy subjects when they are thinking or reading silently, and it has also been demonstrated that patients hearing voices have slight movements of the lips, tongue and laryngeal muscles and that there is an increase in the action potentials in the laryngeal muscles. It is perhaps surprising that more patients do not complain of voices coming from their throat or tongue. Careful investigation of the content and nature of the things that others are alleged to have said may show that the patient has continuous hallucinations and attributes them to real people in the vicinity. As these are often abusive, the patient may attack those whom they believe are responsible. A good example of this was a Greek woman who had been a patient in a longstay ward for many years. She always denied hearing voices but from time to time would make unprovoked attacks on fellow patients. She said that this was not necessary because everybody in the hospital spoke Greek. It became obvious that she heard continuous voices in Greek that she attributed to real people, and that her seemingly motiveless attacks were prompted by this. Vision these may be elementary in the form of flashes of light, partly organised in the form of patterns, or completely organised in the form of visions of people, objects or animals. One patient in delirium tremens described mice carrying suitcases on their backs as they boarded a flight to Lourdes. Scenic hallucinations are common in psychiatric disorders associated with epilepsy, and these patients may also have visions of fire and religious scenes such as the Crucifixion. Sometimes, however, visual and auditory hallucinations co-occur to form a coherent whole. For example, one patient with delirium tremens was very pleased when she saw a tiny German band playing on her counterpane. When these occur in delirium tremens the patient exhibits a combination of child-like pleasure and terror. The disturbance of consciousness makes it difficult for the patient to distinguish between mental images and perceptions, although this is sometimes possible. Some patients with schizophrenia describe visions and these appear to be pseudohallucinations, but on occasion others will insist that their hallucinations are substantial. Imaging studies have demonstrated activity during visual hallucinatory experiences in the extra striate visual areas around the ventral lingual and fusiform gyri (Brodmann area 19), and in the more dorsal cuneus and precuneus regions (Brodmann area 18). It is important to ascertain if they actually smell this odour, since many seem to base their belief on the behaviour of other people who, they say, wrinkle their noses or make reference to the smell. Some patients with schizophrenia claim that they smell gas and that their enemies are poisoning them by pumping gas into the room. Episodes of temporal lobe disturbance are often ushered in by an aura involving an unpleasant odour such as burning paint or rubber. At times, the hallucination may occur without any fit so that the patient then complains of a strange smell in the house. For example, one patient with a temporal lobe focus had no fits but, from time to time, would complain of a smell of stale cabbage water in the house and would turn the house upside down trying to locate the offending object. Sometimes the smell may be pleasant, for example, when some religious people can smell roses around certain saints; this is known as the Padre Pio phenomenon. Depressed patients often describe a loss of taste or state that all food tastes the same. Also, they frequently co-occur with hallucinatory experiences in other modalities including touch and bodily sensation (Langdon et al. Selfsmells (auditory reference syndrome) have also been under-investigated since they are relatively uncommon. The activation was suppressed by treatment with typical antipsychotic agents (Henkin et al. However these patients did not have psychosis and it is not possible to extrapolate these findings to those who may have schizophrenia or other psychiatric disorders. Touch (Tactile) this may take the form of feeling small animals crawling over the body, which is known as formication. Some patients experience feeling cold winds blowing on them, sensations of heat, electrical shocks and sexual sensations; the patient is convinced that these are produced by outside agencies. Indeed, Sims (2003) points out that there is almost always a concomitant delusional elaboration of tactile hallucinatory experiences. Sims (2003) classifies tactile hallucinations into three main types: superficial, kinaesthethic and visceral (see below). Sims further divides superficial hallucinations, which affect the skin, into four types: thermic. Kinaesthetic hallucinations affect the muscles and joints, and the patient feels that their limbs are being twisted, pulled or moved. They occur in schizophrenia, where they can be distinguished from delusions of passivity by the presence of definite sensations. Vestibular sensations such as sinking in the bed or flying through the air can also be hallucinated and are best regarded as a variant of kinaesthetic hallucinations and occur in organic states, most commonly delirium tremens. Some patients with chronic schizophrenia may complain of twisting and tearing pains. These may be very bizarre when the patient complains that his organs are being torn out or the flesh ripped away from his body. For example, a patient described sensations in his brain as of layers of tissue being peeled off so as to bring to completion the battle between good and evil. This may take the form of a delusional belief that there is an animal crawling about in the body. There is also a hallucinatory component since the patient feels it (hallucination) and can describe it in detail. In some cases this is associated with an organic disorder, as in the patient who said he was infested with an animal several centimetres long that he could feel in his stomach. He eventually died and at post-mortem was found to have a tumour invading the thalamus. Most normal people have from time to time the sense that someone is present when they are alone, on a dark street or climbing a dimly lit staircase. Usually this is dismissed as imagination, but nevertheless they look behind them to be certain. However, sometimes there is the feeling that someone is present, whom they cannot see, and whom they may or may not be able to name. This experience was probably the result of lack of sleep, hunger and religious enthusiasm. One patient described a presence over her right shoulder that followed her from room to room and even though she knew that there was nobody there, the feeling was intense and distressing, so much so that at times she hid under the bedclothes to escape. The sense of a presence can occur in healthy people as well as in organic states, schizophrenia or hysteria, and the patient described above also had a diagnosis of borderline personality disorder. Hallucinatory Syndromes Hallucinatory syndromes, also termed hallucinosis, refer to those disorders in which there are persistent hallucinations in any sensory modality in the absence of other psychotic features. They may be threatening or reproachful, although some patients report benign voices. Sensorium is clear, and hallucinations rarely persist longer than one week and are associated with long-standing alcohol misuse. Special Kinds of Hallucination Functional Hallucinations An auditory stimulus causes a hallucination, but the stimulus as well as the hallucination is experienced. For example, a patient with schizophrenia first heard the voice of God as her clock ticked; later, she heard voices coming from the running tap and from the chirruping of the birds. Patients can distinguish both features from each other and crucially, the hallucination does not occur without the stimulus. Some patients who discover that noises induce hallucinatory voices put plugs in their ears to reduce the intensity of the stimulus and hence the hallucinations. One patient recently described that she saw the mouths of her collection of dolls moving. The perception of dolls was necessary to produce the hallucination but the movement of their mouths was distinct and separate and did not represent a transformation of that perception, thus making this a functional hallucination rather than an illusion. Functional hallucinations are not uncommon in chronic schizophrenia and they may be mistaken for illusions. One patient described hearing his own reflection and said that when attempting to carry out some action he could hear himself doing so. In a reflex hallucination, a stimulus in one sensory field produces a hallucination in another. For example, a patient felt a pain in her head (somatic hallucination) when she heard other people sneeze (the stimulus) and was convinced that sneezing caused the pain. Extracampine Hallucinations the patient has a hallucination that is outside the limits of the sensory field. For example, a patient sees somebody standing behind them when they are looking straight ahead, or hears voices talking in London when they are in Liverpool. These hallucinations can occur in healthy people as hypnagogic hallucinations, but also in schizophrenia or organic conditions, including epilepsy. Autoscopy or Phantom Mirror-Image Autoscopy, also called phantom mirror-image, is the experience of seeing oneself and knowing that it is oneself. This symptom can occur in healthy subjects when they are emotionally upset or when exhausted. Occasionally, patients with schizophrenia have autoscopic hallucinations, but these hallucinations are more common in acute and sub-acute delirious states. The organic states most associated with autoscopy are epilepsy, focal lesions affecting the parieto-occipital region and toxic infective states whose effect is greatest in the basal regions of the brain. The fact that autoscopy is often associated with disorders of the parietal lobe due to cerebrovascular disorders or severe infectious diseases accounts for the German folklore belief that when someone sees their double or Doppelganger it indicates that they are about to die. A few patients suffering from organic states look in the mirror and see no image, known as negative autoscopy. Some psychiatrists describe internal autoscopy in which the subject sees their own internal organs, although this is rare. The description of the internal organs is that which would be expected from a layperson, with a crude knowledge of anatomy.
Prostaglandins are intense smooth muscle stimulants that cause intense uterine contractions erectile dysfunction medication list buy viagra with fluoxetine 100/60mg without a prescription. In addition to increase in prostaglandins from endometrial shedding erectile dysfunction drugs from canada buy cheap viagra with fluoxetine on-line, necrosis of endometrial cells provides increased substrate arachidonic acid from cell walls for prostaglandin synthesis impotence young discount viagra with fluoxetine generic. Multiple other factors like behavioral and psychologic factors impotence for erectile dysfunction causes purchase viagra with fluoxetine 100/60mg free shipping, cervical stenosis or narrowing erectile dysfunction and diet buy 100/60 mg viagra with fluoxetine with visa, increased vasopressin release erectile dysfunction lubricant purchase viagra with fluoxetine no prescription, increased uterine activity have been implicated in the cause of primary dysmenorrhea. Secondary dysmenorrhea is caused by structural abnormalities or disease processes that occur outside the uterus, or within the uterine wall or within the uterine cavity. Clinical Presentation Menstrual history should include the age at menarche, cycle regularity, cycle length, last menstrual period, and duration and amount of menstrual flow. Past history: Enquire about previous pelvic infections, pelvic surgeries, injuries, and procedures. Sexual history should include effect of contraceptives on pain, dyspareunia and prior or current history of sexual abuse. Family history should include Endometriosis Physical Examination Pelvic examination focuses on detecting causes of secondary dysmenorrhea. Women with primary dysmenorrhea usually have normal findings on examination and pelvic examination is not usually indicated in young women. In sexually active women the vagina, vulva, and cervix are inspected for lesions and for masses protruding through the external cervical os. Pelvic structures are palpated to check for polyp or fibroid, uterine masses, adnexal masses, thickening of the rectovaginal septum, induration of the cul-de-sac, and nodularity of the uterosacral ligament. Diagnosis of Primary Dysmenorrhea History History of present illness: History should include an assessment of the onset, duration, type, and severity of pain. Clinicians should also ask about the age at which symptoms began, factors that relieve or worsen pain, degree of disruption of daily life, and presence of pelvic pain unrelated to menses. Presence of accompanying symptoms such as cyclic nausea, vomiting, bloating, diarrhea, and fatigue should also be enquired. It usually lasts from 8 to 72 hours and accompanies menstrual flow or precedes it by only a few hours. The pain is associated with other systemic symptoms such as nausea, vomiting, diarrhea, fatigue and headache. Physical examination reveals no abnormality and clinical investigations fail to reveal any underlying pathology. Diagnosis of Secondary Dysmenorrhea By contrast, secondary dysmenorrhea usually occurs years after the onset of menarche and Dysmenorrhea Table 8. The pain is not consistently related to menstruation alone, and may occur throughout the luteal phase of the menstrual cycle. It may also worsen as menses progresses rather than being confined to the first 24 to 48 hours of menstruation. Accompanying symptoms such as an irregular bleeding pattern, heavy periods, vaginal discharge, and dyspareunia can be suggestive of underlying pathology. Physical examination will reveal underlying pelvic pathology which can be confirmed by relevant investigations. Clinical pearl: the diagnosis of secondary dysmenorrhea should be considered when symptoms appear after many years of painless menses. Investigations When the history and clinical examinations are suggestive of primary dysmenorrhea, further investigations are not required. However, further investigations may be necessary in the presence of nonspecific symptoms, abnormal clinical findings, treatment failure of primary dysmenorrhea, or suspicion of secondary dysmenorrhea, or when the diagnosis is in doubt. Further investigations may include the following: Ultrasonography: Uterine leiomyoma, adnexal pathology, endometriomas, and intrauterine contraceptive devices are best assessed with ultrasonography. Cervical culture to exclude sexually transmitted diseases particularly Chlamidya and gonorrhea. Laparoscopy: Helps in the diagnosis of endometriosis, adhesions, and pelvic inflammatory disease and at the same time can offer treatment. Hysteroscopy: May be indicated to evaluate intrauterine pathology if the sonographic findings are unclear. Clinical pearl: Laboratory testing or imaging is not required to make a diagnosis of primary dysmenorrhea. If pain is not relieved with the first agent after two or more cycles at maximum recommended dose, then a second agent may be added. Combined oral contraceptive pills: these are second line treatment if birth control is not desired. The combined oral contraceptive pill inhibits ovulation and leads to thinning of endometrium. This will result in less prostaglandin synthesis with lower level of menstrual fluid volume and thus relief of dysmenorrhea in 90% of women. Other therapies: Other therapies for dysmenorrhea have been proposed, but most are not well studied. These include thiamine, vitamin E, omega-3 fatty acids, magnesium, various herbal medicines, transdermal nitroglycerin, calcium-channel blockers, betaadrenergic agonists, antileukotrienes. Non-pharmacological Treatment Treatment Treatment of primary dysmenorrhea: the treatment of primary dysmenorrhea aims to relieve pain or symptoms. There are three approaches to the management of primary dysmenorrhea: Pharmacological Non-pharmacological Surgical General consideration: the overall approach to management should include skillful manipulation of the psychologic and behavioral factors and the specific pharmacotherapy. Careful assessment of the proportion contributed by the psychologic or reactive component of the pain in dysmenorrhea in each of the patients is essential to appropriate therapy or a combination of therapies. Topical heat: Low level topical heat therapy was as effective as ibuprofen for the treatment of dysmenorrhea. Faster improvement in pain relief was noted when heat therapy was combined with ibuprofen compared with ibuprofen alone. Other therapies: There is limited evidences to support the use acupuncture or spinal nerve stimulation for treatment of dysmenorrhea. Surgical Therapy resection has not been shown to reduce dysmenorrhea and not advocated as mainstream treatment option. However, the risks of laparoscopic documentation must be weighed against the predicted advantages of having a diagnosis of endometriosis when the symptoms are controlled without surgery. Cervical dilatation: Cervical dilatation as a primary method of treatment for primary dysmenorrhea is not warranted. However, dilatation of the cervix should be undertaken when laparoscopies are performed. This surgical manipulation does relieve primary dysmenorrhea temporarily, although with a progressive return of the symptoms. Presacral neurectomy is rarely indicated for treatment of most forms of primary dysmenorrhea. Use of this procedure should be extremely limited and reserved for patients with chronic pelvic pain when other methods of pain relief have failed. However, laparoscopic utero sacral nerve Women wearing the intrauterine device should be treated with nonsteroidal antiinflammatory drugs for their intrauterine device-induced dysmenorrhea and the medication should be given continuously throughout the duration of the menstrual flow. Treatment for most of the other causes of secondary dysmenorrhea should be directed to the specific underlying condition. Surgery has a greater role to play in the treatment of most forms of secondary dysmenorrhea and is usually more definitive. Nonsteroidal antiinflammatory drugs may be given only as a temporary measure to obtain some relief while waiting for surgery. Classification of dysmenorrhea allows practical differentiation in the management of dysmenorrhea 2. Surgical treatment is often required in secondary dysmenorrhea Fill in the blanks 2. Dysmenorrhea Contemporary Issues International Association for the Study of Pain, 2007. Questions for practical (Read the case summary at the beginning of the topic before answering the questions) 1. The symptoms had improved when she was on oral contraceptives following her marriage three years ago. Recently these symptoms have become more troublesome, interfering with her relationship with husband and her ability to perform optimally at work as school teacher. Physical examination reveals normal findings with normal breast and pelvic examination. Etiopathology: the etiology of premenstrual syndrome remains unknown and may be complex and multifactorial. Cyclicity and physiologic hormonal variations of estrogen and progesterone make an impact on central neurotransmitters which seem to be the basis of the condition. Symptoms: Common symptoms are abdominal bloating, breast tenderness, and headaches. Symptoms may include the following: Feeling sad, hopeless, or self-deprecating Tension, anxiety, mood liability, fearfulness, or persistent irritability Anger Decreased interest in usual activities Difficulty in concentrating Feeling fatigued Changes in appetite Hypersomnia or insomnia Feeling overwhelmed or out of control Other physical symptoms such as headaches, breast tenderness, or swelling, joint or muscle pain, bloating or weight gain. At least one symptom must be among the first four listed: Depressed mood Significant anxiety Affective lability Persistent anger or irritability Decreased interest in usual activities Concentration difficulty Lethargy Change in eating habits Insomnia or hypersomnia Sense of being overwhelmed Other physical symptoms such as headache, breast tenderness, bloating or weight gain. Pharmacotherapy: Two primary approaches are used when symptoms are not relieved by lifestyle modification only. Rarely, for very severe or refractory symptoms, a gonadotropin-releasing hormone agonist. Anxiolytics such as alprazolam may be indicated as second-line therapy for refractory behavioral symptoms. Other therapies: Evening primrose oil is a popular self-treatment, but trials are of poor quality. Treatment the aim of treatment is to provide relief of symptoms during leuteal phase and to improve quality of life. Regular exercise may help alleviate bloating as well as irritability, anxiety, and insomnia. Dietary changes-increasing protein, decreasing sugar, and taking vitamin B complex (especially pyridoxine, a form of vitamin B6) or Mg supplements-may help. Fluid retention may be relieved by reducing Na 74 Essentials in Gynecology Clinical pearl: Good, level I evidence supports using calcium carbonate and selective serotonin reuptake inhibitors. Less conclusive evidence suggests some relief with aerobic exercise, high-complex carbohydrate diets, stress reduction, spironolactone for swelling, magnesium, nonsteroidal anti-inflammatory drugs, hormone treatment, evening primrose oil, oral contraceptives, and vitamins B6 and E. It offers a common language and standard criteria for the classification of mental disorders. Presence of premenstrual symptoms is not adequate enough to diagnose premenstrual syndrome 2. Premenstrual syndrome 10 Primary Amenorrhea A 16-year-old teenage girl has not started menstruation yet, while her elder has started her first period at age 13. Physical exam shows breast development at Tanner stage 2, external genitalia at Tanner stage 1. However, if the patient has no sign of secondary sexual development, this is abnormal and demands further investigation. Fact sheet: Historical treatment of primary amenorrhea often consisted of ammonia injections into the vagina, as the intense pain was thought to stimulate normal menstrual cycles. However, we must remember that whichever way we classify causes of primary amenorrhea, there will be always an overlap of condition from one compartment to another. Secondary sexual development is good apart from amenorrhea (Presence of breast development indicates production of estrogen at one point of time): the causes are: a. Some women with constitutional delay in puberty Now let us further divide the causes- anatomic defects of outflow tract may be due to: a. If secondary sex character development is poor or absent (absent breast development indicates lack of estrogen production), the causes can be a. Clinicians need to consider the young age and emotional maturity of the patient when examining the adolescent. History and physical examinations frequently direct the clinician towards a working diagnosis; however, ancillary studies are often necessary. Breast development, pubertal growth spurt, and adrenarche are delayed or absent in girls with hypothalamic pituitary failure. In case of isolated ovarian failure, adrenarche occurs normally, while estrogen-dependent breast development and the pubertal growth spurt are absent or delayed. Most systemic disorders may be diagnosed with laboratory tests assessing neuroendocrine and ovarian function, and the majority of structural abnormalities are identified through pelvic examination or imaging studies. History Complaint A history of cyclic pelvic pain in association with primary amenorrhea suggests the possibility of a congenital outflow tract abnormality such as imperforate hymen or agenesis of the vagina, cervix. Associated galactorrhea, headaches, or reduced peripheral vision could be a sign of intracranial tumor such as prolactinoma. An impaired sense of smell in association with primary amenorrhea and failure of normal pubertal development may be related to isolated gonadotropin deficiency, Primary Amenorrhea 77 as is observed in persons with Kallmann syndrome. Medical History Chronic systemic illness may present with fatigue, malaise, anorexia, and weight loss. Dieting with excessive restriction of energy intake, especially fat restriction, may lead to amenorrhea and associated bone loss. Past History History of a traumatic head injury or infection: A remote history may be elicited from the patient or parents.

















