

Prem Puri, MS, FRCS, FRCS (Ed), FACS, FAAP (Hon)
- Newman Clinical Research Professor,
- School of Medicine and Medical Science, University College
- Dublin
- Consultant Paediatric Surgeon and Director of
- Research, Children? Research Centre, Our Lady? Children?
- Hospital, Dublin, Ireland
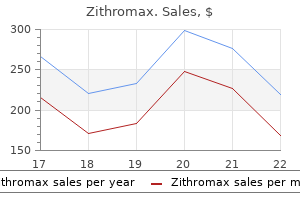
Arterial flow varies with the cardiac cycle antibiotic 1338 zithromax 100mg otc, with a rapid rise to peak velocity during systole bacteria facts for kids cheap zithromax 500mg free shipping, and gradual decrease in velocity during diastole antibiotics for uti baby buy 250 mg zithromax overnight delivery. The normal Doppler waveform in high-resistance arteries is stenosis shows increased velocity and broadening of the waveform in the region of greatest arterial narrowing (arrow) bacteria gram stain cheap 500 mg zithromax fast delivery. The normal Doppler waveform in a low-resistance visceral artery is biphasic: fast antegrade flow during systole with slower antegrade flow during diastole antimicrobial drugs antibiotics buy zithromax with amex. The velocity and pulsation vary depending on the proximity of the vein to the heart antibiotic gel for acne zithromax 100mg sale, the health of the heart, and the volume status of the patient. Phasic changes in velocity with respiration also occurs, with substantial increases in flow during inspiration and dampened flow during expiration. The color of the flow is determined by how the operator holds the transducer; one should never try to identify a vessel based on color alone. The color image is superimposed upon a grayscale image to provide anatomic definition, and many ultrasound machines also allow simultaneous display of a pulsed-wave tracing. Power Doppler uses the overall energy in the Doppler signal to assign color, without regard for the magnitude of the phase shift (velocity) or direction. Since the majority of the signal is created by moving red blood cells, this technique is more sensitive to flow than standard color imaging. Although this is useful when evaluating areas of slow flow or small structures, other movement such as transmitted pulsations or vibrations will also be more apparent on the images. NoNiNvasive vascular imagiNg 59 Ultrasound imaging has several limitations, some of which are related to the physics of the technique, and some to the person performing the examination. Complex nonlinear structures must be evaluated in a piecemeal fashion, with intense concentration upon the part of the examiner in order to perform a complete study. Doppler imaging has several key weaknesses, including unreliable velocity calculations when the angle of insonation is greater than 60 degrees, as described earlier. Very slow flow is difficult to detect, particularly in deep vessels, which may lead to the false conclusion that a vessel is occluded, a potentially serious error when evaluating the carotid arteries. On the other hand, extremely fast flow may exceed the ability of a particular ultrasound machine to measure or display the velocity, but this is rarely an important problem in patient management. Furthermore, because color-encoding is determined by the operator, the identity of a vessel cannot be assumed from the color of the flow. In general, 2-D imaging provides excellent vascular signal at the expense of image resolution, whereas 3-D imaging provides better resolution (thinner slices) but is susceptible to signal loss as volumes increase in size. The use of ultrasound contrast for vascular imaging is less common, but has been described in the follow-up of abdominal aortic endografts. Application of an additional radiofrequency pulse to the protons tips the spins out of alignment with the magnetic field in a plane perpendicular to the magnetic field (transverse magnetization). The natural tendency of the protons is to realign themselves with the magnetic field (relaxation), which creates a detectable signal (echo). These signal characteristics can change with the presence of pathology or bleeding, or following administration of a contrast agent. Fast flow in the true lumen is black (straight arrow), slow flow in the false lumen is gray (arrowhead), and chronic mural thrombus in the false lumen is bright (curved arrow). The artery may be occluded, severely stenotic with such slow flow that signal is suppressed along with the background tissues, or have reversed flow that is saturated along with the venous flow. The gadolinium contrast agent is injected rapidly through a peripheral vein, with image acquisition timed to occur as the contrast enters the arterial circulation in the region of interest. Although 3-D volumes are routinely used, there is no loss of signal due to saturation effects as experienced with noncontrast techniques. There are fewer adverse reactions to gadolinium contrast agents than with iodinated contrast, and gadolinium appears to have little clinical nephrotoxicity. Patients with most cardiac pacemakers, defibrillators, intraocular or intraaural metallic foreign bodies, or claustrophobia cannot be imaged. Gadolinium-enhanced 3-D magnetic resonance angiogra- phy of the aorta and bilateral lower extremity arteries in a patient with peripheral arterial disease. Time-resolved gadolinium-enhanced imaging of the tibial arteries in a patient with peripheral arterial disease, displayed as maximum intensity projection images. When creating study protocols, keep in mind that the thinner the collimation or greater the pitch, the lower the ratio of signal to noise in the image. Multiple interweaving helices are acquired at the same time, allowing reduced scan times, reduced volumes of contrast, reduced motion and pulsatility artifacts, and improved spatial resolution. Slice thickness is determined by the thickness of the detector elements rather than beam collimation, and may be substantially less than 1 mm. B, Digital subtraction angiography of the distal abdominal aorta and pelvis demonstrates a stent in the left common iliac artery (arrow) that has mild proximal in-stent restenosis but is otherwise patent. A, Single slice from a gadolinium-enhanced 3-D magnetic resonance angiography of the aortic arch obtained during injection of contrast through a left upper extremity vein. There is a signal void in the left brachiocephalic vein (arrow) with surrounding susceptibility artifact causing an apparent bulky eccentric stenosis of the adjacent brachiocephalic artery. The patient had treatment of a thoracoabdominal aneurysm with surgical bypasses to the celiac, superior mesenteric artery, and right renal artery from the left common iliac artery (arrow) and placement of endografts (arrowhead) from the thoracic aorta to the infrarenal abdominal aorta. Computed Tomography Angiography Advantages Large field of view Vascular enhancement by contrast Rapid scan time allowing extensive longitudinal coverage (whole-body scan) Limited number of variables to manipulate Valuable information in source images Scanners readily available Conventional monitoring/respiratory equipment usable Box 3-4. Small, heavily calcified vessels are difficult to evaluate, because bulky intimal calcium can be indistinguishable from the opacified vessel lumen. If an image is constructed of large rectangular voxels, small objects may get "lost" (partial volume averaging), particularly when viewed from a perspective perpendicular to the long axis of the voxel. Strengths Quick; no loss of data; can display complex anatomy Quick; bright vessels 3-D-like rendition of selected voxel values while retaining complete data set Allows viewer to enter and travel through lumen of blood vessel Weaknesses Overlap of structures can be confusing, 2-D display only Threshold for display may result in loss of critical information; 2-D display only Threshold for model may render critical voxels transparent Intraluminal perspective only Allows display of all data in volume in user-defined 2-D planes, including curved Displays brightest voxels in user-defined 2-D planes; discards background information Displays voxels as a virtual 3-dimensional volume; objects selected by setting threshold, opacity values Displays tubular structures without intraluminal contents with 3-D appearance Endoscopic transparent or discarded. The remaining voxels are then manipulated to enhance the appearance of the final images, often by adding or further subtracting data as needed. For these reasons, all 3-D models must be viewed with some skepticism and correlated to the axial images, because important information can be omitted at several stages during creation of the final images (Box 3-5). The brightest pixels are summated so that the arteries are displayed in a single image, but there is loss of much of the source image data. Guidelines for noninvasive vascular laboratory testing: a report from the American Society of Echocardiography and the Society for Vascular Medicine and Biology. The history of percutaneous catheter-based vascular interventions mirrors the development of interventional radiology as a specialty. Diagnostic angiography was originally just one of the several imaging technologies (albeit the most invasive) used by radiologists to obtain diagnostic images for other physicians. Interventional radiology has grown to include the clinical management of patients undergoing image-guided therapy and focused areas of diseasespecific practice such as oncology and peripheral vascular disease. A variety of strategies have been devised to restore patency of both arteries and veins, but all have certain elements in common (Box 4-1). For example, short concentric noncalcified atherosclerotic lesions usually respond well to simple angioplasty, whereas long, calcified occlusions may be impossible to cross or dilate. If a large sheath will be required, consider partially deploying a suture-mediated closure device before the sheath is inserted (see Box 2-10). The patient should be anticoagulated with unfractionated heparin or bivalirudin just before or immediately after crossing the lesion. Distinguishing between the two is essential; filling of normal caliber lumen and branches indicates successful crossing of the lesion, whereas focal pooling of contrast or tracking around a central unopacified lumen indicates a subintimal location. To gain access to the occluded lumen, an angled or straight catheter is advanced up to the cap and a guidewire is then used to probe for a "soft spot. When the initial attempts to cross the occlusion fail, different shaped catheters and guidewires with gradually increased stiffness are used. This lesion is difficult to treat with angioplasty alone because the normal wall opposing the lesion will stretch and recoil with balloon inflation. If this occlusion is due to fresh thrombus within the lesion, consider thrombolysis or mechanical thrombectomy before treating the underlying stenosis. The proposed benefits of this approach are the absence of atheromatous disease in the media and the ability to recanalize extremely long distances, such as groin to ankle. B, Retrograde injection of contrast after stent placement (arrow) shows an occlusion of the common iliac artery proximal to the stent and subintimal contrast (arrowheads) outlining the infrarenal aorta. The guidewire spontaneously reenters the true lumen distally at the interface of the plaque and normal intima in approximately two thirds of the procedures. After confirming successful navigation across the lesion by aspirating blood or injecting contrast, a working guidewire is advanced through the catheter to provide stability for the intervention. In general, relatively stiff guidewires are used that allow devices to be advanced into position without losing access across the lesion. Hydrophilic coated guidewires are usually not a good choice for working wires, because they easily slip out of place during catheter exchanges. The final desired diameter of a blood vessel is determined from an adjacent normal segment of vessel, the same vessel on the other side of the body in the case of bilateral structures or the known average size of the vessel. When measuring directly from images, it is helpful to calibrate to a known internal standard such as a marker catheter or guidewire, but this method is not always accurate. The vessel and the type of lesion also impact sizing, in that veins are usually more compliant, whereas heavily calcified arteries may fracture when overdilated. The length of the device should be sufficient to treat the diseased area, with minimal trauma to adjacent normal or slightly diseased vessels. When the area of disease to be treated extends up to or across a bifurcation into a smaller diameter vessel, the device should be sized or delivered in a manner that avoids trauma to the smaller or normal vessel. Because the clinical outcome cannot always be measured during a procedure, most interventionalists use technical endpoints such as a residual luminal stenosis of less than 20% or reduction of the pressure gradient across the lesion to a predetermined level. In many instances a catheter must be through the lesion of interest in order to obtain a distal pressure, such as in the renal artery. Specialized pressure-sensing guidewires may be useful in these cases, but in general most interventionalists believe that any symptomatic lesion tight enough to be partially obstructed by an angiographic catheter requires treatment. The hollow curved needle (arrow) is used to puncture from one lumen to the other, through which a guidewire can be advanced into the newly entered lumen. The right renal artery stenosis (white arrow) is so tight that the remainder of the right renal artery (also with post-stenotic dilation) is barely opacified. Older patients with acute illnesses, diffuse vascular disease, and concurrent major illnesses are most likely to experience a complication. Most early failures are due to technical issues such as an occlusive dissection adjacent to the intervention site that impedes flow, elastic recoil of a fibrotic lesion, or perhaps a missed lesion that continues to impair flow. Hypercoagulable syndromes, episodes of hypotension, or other low-flow states can result in acute thrombosis at arterial or venous intervention sites at any time. The patient had notable pain (7 out of 10) with balloon inflation, so the operator did not try to dilate the stents further for fear of rupturing an artery. Drug-eluting balloons, drug-eluting stents, and stent-grafts show promise for improved long-term clinical success rates in various vascular applications. There is evidence suggesting that antiplatelet and statin therapies may reduce restenosis rates following peripheral arterial interventions. After 1 year, failure of a revascularization procedure is more likely to be due to progression of the original disease in the inflow or outflow vessels. Noncompliant balloons reach a nominal predetermined diameter during inflation and remain close to that diameter as pressure is increased to the bursting point (many of these balloons actually increase slightly in diameter as pressure increases). Noncompliant balloons are desirable for angioplasty; otherwise the balloon expands on either side of the waist without dilating the stenosis. Very high pressure noncompliant balloons (up to 30 atm) are used in venous and nonvascular applications, whereas lower pressure balloons are used in arterial lesions. A balloon that ruptures before the lesion is fully dilated is of little value, but a balloon that is so strong that the vessel ruptures first is potentially dangerous. This results in formation of fissures in the plaque itself, and tearing of the edges of the plaque away from the adjacent normal intima. Compliant balloons are constructed from material that continues to stretch as pressure is applied, allowing the balloon to expand until the Box 4-4. The distal portion (arrow) detached from the catheter in the vascular system during attempted extraction because the balloon membrane mushroomed and jammed against the tip of the sheath. Latex occlusion balloon (left); 8-mm Popliteal artery Tibial artery Pedal artery Superior vena cava Subclavian/brachiocephalic vein Brachial/basilic veins Iliac veins *These sizes serve as a rough guide; measurements from reliable imaging should always be used when possible for selection of balloon dimensions. An initially undersized balloon rarely causes a complication, and a larger balloon can always be used if the result is unsatisfactory. Because of the physics of balloons (tension = pressure Ч radius), the larger the balloon, the lower the necessary inflation pressure. Dilute contrast (1 part contrast to 2-3 parts flush solution) is used for inflation to allow visualization of the balloonlesion interaction and facilitate rapid deflation. The guidewire exits the catheter (arrow) near the balloon end, so only a small portion of this 150 cm long catheter travels over the guidewire. In the hands of most humans, a 10-mL Luer-lock syringe can maximally generate 10-12 atm, which is sufficient to dilate the majority of arterial lesions. A mechanical inflation device or a smaller syringe (5 or 3 mL) can be used to generate the higher pressures sometimes needed for fibrotic or venous lesions. Angioplasty balloons are mounted on angiographic catheters, usually with two lumens: one for a guidewire and one for balloon inflation/deflation. The back end of the standard over-the-wire balloon catheter usually has two separate Luer-lock hubs, one for the central guidewire lumen and one for balloon inflation. This allows for lower catheter profiles and insertion of a long catheter over a standard length guidewire, because the majority of the catheter slides alongside the guidewire, not over it. When removing a balloon through a sheath, resistance may be encountered because the deflated balloon does not return to its original low profile. Continued aspiration and counterclockwise rotation as the catheter is withdrawn into the sheath rewraps the balloon around the shaft and facilitates removal.
For example bacteria mrsa purchase zithromax 100mg with visa, the increasing incidence of obesity in the United States and other industrialized nations during the past 40 years cannot be explained by changes in our genes antibiotics for sinus infection safe while breastfeeding generic 100 mg zithromax amex. Much recent research has focused on possible abnormalities in the leptin system as a cause of obesity antibiotics for dogs buy buy zithromax 100mg otc. In one strain of mice (shown in the chapter-opening photo) treatment for uti medications effective 250mg zithromax, the gene that codes for leptin is mutated so that adipose-tissue cells produce an abnormal virus going around schools purchase cheapest zithromax and zithromax, inactive leptin infection joint pain discount 100 mg zithromax with amex, resulting in hereditary obesity. The leptin secreted by these people is normal, and leptin concentrations in the blood are increased, not decreased. Consequently, such people are leptin-resistant in much the same way that people with type 2 diabetes mellitus are insulin-resistant. The methods and goals of treating obesity are now undergoing extensive rethinking. An increase in body fat must be due to an excess of energy intake over energy expenditure, and low-calorie diets have long been the mainstay of therapy. However, it is now clear that such diets alone have limited effectiveness in obese people; over 90% regain all or most of the lost weight within 5 years. Because of this, many obese people continue to gain weight or remain in stable energy balance on a caloric intake equal to or less than the amount consumed by people of normal weight. These persons must either have less physical activity than normal or have lower basal metabolic rates. Finally, at least half of obese people - those who are more than 20% overweight - who try to diet down to desirable weights suffer medically, physically, and psychologically. This is what would be expected if the body were "trying" to maintain body weight (more specifically, fat stores) at the higher set point. Such studies, taken together, indicate that crash diets are not an effective long-term method for controlling weight. Such an intake in an overweight person should lead to a slow, steady weight loss of no more than 1 pound per week until the body weight stabilizes at a new, lower level. The most important precept is that any program of weight loss should include increased physical activity. The exercise itself uses calories, but more importantly, it partially offsets the tendency, described earlier, for the metabolic rate to decrease during long-term caloric restriction and weight loss. Also, the combination of exercise and caloric restriction may cause the person to lose more fat and less protein than with caloric restriction alone, although some recent studies suggest this may not always be true. Let us calculate how rapidly a person can expect to lose weight on a reducing diet (assuming, for simplicity, no change in energy expenditure). Suppose a person whose steady-state metabolic rate per 24 h is 2000 kcal goes on a 1000 kcal/day diet. Therefore, even on this severe diet, the person can reasonably expect to lose approximately this amount of weight per week, assuming no decrease in metabolic rate occurs. Eating Disorders: Anorexia Nervosa and Bulimia Nervosa Two of the major eating disorders are found primarily in adolescent girls and young women. The typical person with anorexia nervosa becomes pathologically obsessed with her weight and body image. There are many other abnormalities associated with anorexia nervosa - cessation of menstrual periods, low blood pressure, low body temperature, and altered secretion of many hormones, including increased concentrations of ghrelin. It is likely that these are simply the results of starvation, although it is possible that some represent signs, along with the eating disturbances, of primary hypothalamic malfunction. Bulimia nervosa, usually called simply bulimia, is a disorder characterized by recurrent episodes of binge eating. It is usually associated with regular self-induced vomiting and use of laxatives or diuretics, as well as strict dieting, fasting, or vigorous exercise to lose weight or to prevent weight gain. Like individuals with anorexia nervosa, those with bulimia manifest a persistent heightened concern with body weight, although they generally remain within 10% of their ideal weight. This disorder too, is accompanied by a variety of physiological abnormalities, but it is unknown in some cases whether they are causal or secondary. In addition to anorexia and bulimia, rare lesions or tumors within the hypothalamic centers that normally regulate appetite can result in overfeeding or underfeeding. In recent years, more and more dietary factors have been associated with the cause or prevention of many diseases or disorders, including not only coronary artery disease but hypertension, cancer, birth defects, osteoporosis, and others. These associations come mainly from animal studies, epidemiologic studies on people, and basic research concerning potential mechanisms. One of the most commonly used sets of dietary recommendations, issued by the National Research Council, is presented in Table 16. Reduce saturated fatty acid intake to less than 10% of calories and intake of cholesterol to less than 300 mg daily. Every day eat five or more servings of a combination of vegetables and fruits, especially green and yellow vegetables and citrus fruits. Also, increase complex carbohydrates by eating six or more daily servings of a combination of wholegrain breads, cereals, and legumes. For those who drink alcoholic beverages, limit consumption to the equivalent of 1 ounce of pure alcohol in a single day. Maintain an optimal intake of fluoride, particularly during the years of primary and secondary tooth formation and growth. Rectal temperature (°C) Summary of National Research Council Dietary Recommendations 37. This figure does not take into account daily minor swings in temperature due to such things as exercise, eating, and menstrual cycle; nor are the absolute values on the y-axis representative of all individuals. The total heat content gained or lost by the body is determined by the net difference between heat gain (from the environment and produced in the body) and heat loss. Maintaining a stable body temperature means that, in the steady state, heat gain must equal heat loss. In this section, we discuss the mechanisms by which the body gains or loses heat in a variety of healthy or pathological settings. Humans are endotherms, meaning that they generate their own internal body heat and do not rely on the energy of sunlight to warm the body. Moreover, humans maintain their body temperatures within very narrow limits despite wide fluctuations in ambient temperature and are, therefore, also known as homeotherms. The relatively stable body temperature frees biochemical reactions from fluctuating with the external temperature. However, the maintenance of a warm body temperature (approximately 378C in healthy persons) imposes a requirement for precise regulatory mechanisms because large elevations of temperature cause nerve malfunction and protein denaturation. Some people suffer convulsions at a body temperature of 418C (1068F), and 438C is considered to be the absolute limit for survival. A few important generalizations about normal human body temperature should be stressed at the outset. Before defining each of these processes, however, it must be emphasized that radiation, conduction, and convection can, under certain circumstances, lead to heat gain instead of loss. Radiation is the process by which the surfaces of all objects constantly emit heat in the form of electromagnetic waves. It is a principle of physics that the rate of heat emission is determined by the temperature of the radiating surface. As a result, if the body surface is warmer than the various surfaces in the environment, net heat is lost from the body, the rate being directly dependent upon the temperature difference between the surfaces. Conversely, the body gains heat by absorbing electromagnetic energy emitted by the sun. Conduction is the loss or gain of heat by transfer of thermal energy during collisions between adjacent molecules. The body surface loses or gains heat by conduction through direct contact with cooler or warmer substances, including the air or water. Water is a better conductor of heat than is air; therefore, more heat is lost from the body in water than in air of similar temperature. Convection is the process whereby conductive heat loss or gain is aided by movement of the air or water next to the body. Radiation Convection Warm air rising Evaporation Cool air coming in to replace warm air that has risen Conduction Water temperature greater than body temperature effectors so that heat production and/or loss are modified and body temperature is restored toward normal. There are two locations of thermoreceptors, one in the skin (peripheral thermoreceptors) and the other (central thermoreceptors) in deep body structures, including abdominal organs and thermoreceptive neurons in the hypothalamus. Because it is the core body temperature - not the skin temperature - that is maintained in a narrow homeostatic range, the central thermoreceptors provide the essential negative feedback component of the reflexes. The peripheral thermoreceptors provide feedforward information, as described in Chapter 1, and also account for the ability to identify a hot or cold area of the skin. The hypothalamus serves as the primary overall integrator of the reflexes, but other brain centers also exert some control over specific components of the reflexes. Output from the hypothalamus and the other brain areas to the effectors is via (1) sympathetic nerves to the sweat glands, skin arterioles, and the adrenal medulla; and (2) motor neurons to the skeletal muscles. Because warm air is less dense than cool air, the heated air around the body surface rises, thereby carrying away the heat just taken from the body. The air that moves away is replaced by cooler air, which in turn follows the same pattern. Convection is always occurring because warm air is less dense and therefore rises, but it can be greatly facilitated by external forces such as wind or fans. Consequently, convection aids conductive heat exchange by continuously maintaining a supply of cool air. Therefore, in the rest of this chapter, the term conduction will also imply convection. Evaporation of water from the skin and membranes lining the respiratory tract is the other major process causing loss of body heat. A very large amount of energy - 600 kcal/L - is required to transform water from the liquid to the gaseous state. Temperature-Regulating Reflexes Temperature regulation offers a classic example of a homeostatic control system, as described in Chapter 1. The balance between heat production (gain) and heat loss is continuously being disturbed, either by changes in metabolic rate (exercise being the most powerful influence) or by changes in the external environment such as air temperature. These receptors initiate reflexes that change the output of various Changes in muscle activity constitute the major control of heat production for temperature regulation. The first muscle change in response to a decrease in core body temperature is a gradual and general increase in skeletal muscle contraction. This may lead to shivering, which consists of oscillating, rhythmic muscle contractions and relaxations occurring at a rapid rate. During shivering, the efferent motor nerves to the skeletal muscles are influenced by descending pathways under the primary control of the hypothalamus. Because almost no external work is performed by shivering, most of the energy liberated by the metabolic machinery appears as internal heat, a process known as shivering thermogenesis. People also use their muscles for voluntary heatproducing activities such as foot stamping and hand rubbing. Basal muscle contraction is reflexively decreased, and voluntary movement is also diminished. These attempts to decrease heat production are limited, however, because basal muscle contraction is quite low to start with and because any increased core temperature produced by the heat acts directly on cells to increase metabolic rate. In other words, an increase in cellular temperature directly accelerates the rate at which all of its chemical reactions occur. This is due to the increased thermal motion of dissolved molecules, making it more likely that they will encounter each other. Thus, increasing cellular temperature can itself result in the production of additional heat through increased metabolism. Muscle contraction is not the only process controlled in temperature-regulating reflexes. In many experimental mammals, chronic cold exposure induces an increase in metabolic rate (and therefore heat production) that is not due to increased muscle activity and is termed nonshivering thermogenesis. The dashed arrow from the adrenal medulla indicates that this hormonal pathway is of minor importance in adult human beings. This type of adipose tissue is stimulated by thyroid hormone, epinephrine, and the sympathetic nervous system; it contains large amounts of a class of proteins called uncoupling proteins. The major product of this inefficient metabolism is heat, which then contributes to maintaining body temperature. Nonshivering thermogenesis does occur in infants, therefore, whose shivering mechanism is not yet fully developed. Control of Heat Loss by Radiation and Conduction For purposes of temperature control, the body may be thought of as a central core surrounded by a shell consisting of skin and subcutaneous tissue. The temperature of the central core is regulated at approximately 378C, but the temperature of the outer surface of the skin changes considerably. If the skin and its underlying tissue were a perfect insulator, no heat would ever be lost from the core. The temperature of the outer skin surface would equal the environmental temperature, and net conduction would be zero. The skin is not a perfect insulator, however, so the temperature of its outer surface generally is somewhere between that of the external environment and that of the core. Instead of acting as an insulator, the skin functions as a variable regulator of heat exchange. Its effectiveness in this capacity is subject to physiological control by a change in blood flow. In effect, the blood vessels can carry heat to the skin surface to be lost to the external environment. These vessels are controlled 594 Chapter 16 largely by vasoconstrictor sympathetic nerves, which are reflexively stimulated in response to cold and inhibited in response to heat.
Purchase zithromax online pills. Public Health Support for Antimicrobial Stewardship.
In Chapter 4 prophylactic antibiotics for uti guidelines 500mg zithromax otc, we described how a net movement of water occurs across a semipermeable membrane from a solution of high water concentration to a solution of low water concentration antibiotic resistance dangerous buy discount zithromax 100 mg online. Stated another way bacteria background purchase zithromax 250 mg with amex, water moves from a region with a low concentration of nonpenetrating solute to a region with a high concentration of nonpenetrating solute treatment for uti keflex buy cheap zithromax line. Moreover antibiotic jokes purchase 500mg zithromax with visa, this osmotic flow of water "drags" along with it solutes that can penetrate the membrane antibiotic for uti proteus trusted zithromax 250 mg. Thus, a difference in water concentration secondary to different concentrations of nonpenetrating solute on the two sides of a membrane can result in the movement of a solution containing both water and penetrating solutes in a manner similar to the bulk flow produced by a hydrostatic pressure difference. Units of pressure (mmHg) are used in expressing this osmotic force across a membrane, just as for hydrostatic pressures. The plasma within the capillary and the interstitial fluid outside it contain large quantities of lowmolecular-weight solutes (also termed crystalloids) that easily penetrate capillary pores. Because these crystalloids pass easily through the capillary wall, their concentrations in the plasma and interstitial fluid are essentially identical. Consequently, the presence of the crystalloids causes no significant difference in water concentration. In contrast, the plasma proteins (also termed colloids) are unable to move through capillary pores (nonpenetrating) and have a very low concentration in the interstitial fluid. The difference in protein concentration between the plasma and the interstitial fluid means that the water concentration of the plasma is slightly lower (by about 0. Because the crystalloids in the interstitial fluid move along with water, flow that is driven by either osmotic or hydrostatic pressures across the capillary wall does not alter crystalloid concentrations in either plasma or interstitial fluid. The amount of water (the volume) and the amount of crystalloids in the two locations do change. Thus, an increased filtration of fluid from plasma to interstitial fluid increases the volume of the interstitial fluid and decreases the volume of the plasma, even though no changes in crystalloid concentrations occur. The four factors that determine net filtration pressure are termed the Starling forces because Starling, the same physiologist who helped elucidate the FrankStarling mechanism of the heart, was the first to describe these forces. Much of the arterial blood pressure has already dissipated as the blood flows through the arterioles, so that hydrostatic pressure tending to push fluid out of the arterial end of a typical capillary is only about 35 mmHg. The interstitial fluid protein concentration at this end of the capillary would produce a flow of fluid out of the capillary equivalent to a hydrostatic pressure of 3 mmHg. Because the interstitial fluid hydrostatic pressure is virtually zero, the only inward-directed pressure at this end of the capillary is the osmotic pressure due to plasma proteins, with a value of 28 mmHg. At the arterial end of the capillary, therefore, the net outward pressure exceeds the inward pressure by 10 mmHg, so bulk filtration of fluid will occur. The only substantial difference in the Starling forces at the venous end of the capillary is that the hydrostatic blood pressure (Pc) has decreased from 35 to approximately 15 mmHg due to the resistance encountered as blood flowed along the capillary wall. The other three forces are virtually the same as at the arterial end, so the net inward pressure is about 10 mmHg greater than the outward pressure, and bulk absorption of fluid into the capillaries will occur. Thus, net movement of fluid from the plasma into the interstitial space at the arterial end of capillaries tends to be balanced by fluid flow in the opposite direction at the venous end of the capillaries. Outward forces are arbitrarily assigned positive values, so a positive net filtration pressure favors filtration, whereas a negative pressure indicates that net absorption of fluid will occur. In our example, we have assumed a typical capillary hydrostatic pressure varying from 35 mmHg down to 15 mmHg. In reality, capillary hydrostatic pressures vary in different regions of the body and, as will be described in a later section, are strongly influenced by whether the person is lying down, sitting, or standing. Moreover, capillary hydrostatic pressure in any given region is subject to physiological regulation, mediated mainly by changes in the resistance of the arterioles in that region. Cardiovascular Physiology 401 of the increased capillary hydrostatic pressure, filtration is increased and more protein-free fluid is transferred to the interstitial fluid. In contrast, marked arteriolar constriction produces decreased capillary hydrostatic pressure and favors net movement of interstitial fluid into the vascular compartment. Indeed, the arterioles supplying a group of capillaries may be so dilated or so constricted that the capillaries manifest only filtration or only absorption, respectively, along their entire length. To reiterate an important point, capillary filtration and absorption play a minimal role in the exchange of nutrients and metabolic end products between capillaries and tissues. The reason is that the total quantity of a substance, such as glucose or carbon dioxide, moving into or out of a capillary as a result of net bulk flow is extremely small in comparison with the quantities moving by net diffusion. Finally, this analysis of capillary fluid dynamics has considered only the systemic circulation. The same Starling forces apply to the capillaries in the pulmonary circulation, but the relative values of the four variables differ. In particular, because the pulmonary circulation is a lowresistance, low-pressure circuit, the normal pulmonary capillary hydrostatic pressure - the major force favoring movement of fluid out of the pulmonary capillaries into the interstitium - averages only about 7 mmHg. This is offset by a greater accumulation of proteins in lung interstitial fluid than is found in other tissues. Overall, the Starling forces in the lung slightly favor filtration as in other tissues, but extensive and active lymphatic drainage prevents the accumulation of extracellular fluid in the interstitial spaces and airways. In some pathophysiological circumstances, imbalances in the Starling forces can lead to edema - an abnormal accumulation of fluid in the interstitial spaces. Heart failure (discussed in detail in Section E) is a condition in which increased venous pressure reduces blood flow out of the capillaries, and the increased hydrostatic pressure (Pc) causes excess filtration and accumulation of interstitial fluid. A more common experience is the swelling that occurs with injury - for example, when you sprain an ankle. In addition, the chemicals released within injured tissue cause endothelial cells to distort, increasing the size of intercellular clefts and allowing plasma proteins to escape from the bloodstream more readily. Finally, an abnormal decrease in plasma protein concentration also can result in edema. This condition reduces the main absorptive force at capillaries (c), thereby allowing an increase in net filtration. Plasma protein concentration can be reduced by liver disease (decreased plasma protein production) or by kidney disease (loss of protein in the urine). In addition, as with liver disease, protein malnutrition (kwashiorkor) compromises the manufacture of plasma proteins. The resulting edema is particularly marked in the interstitial 402 Chapter 12 spaces within the abdominal cavity, producing the swollenbelly appearance commonly observed in people with insufficient protein in their diets. Some exchange of materials occurs between the interstitial fluid and the venules, just as in capillaries. Indeed, permeability to macromolecules is often greater for venules than for capillaries, particularly in damaged areas. The veins are the last set of tubes through which blood flows on its way back to the heart. In the systemic circulation, the force driving this venous return is the pressure difference between the peripheral veins and the right atrium. The pressure in the first portion of the peripheral veins is generally quite low - only 10 to 15 mmHg - because most of the pressure imparted to the blood by the heart is dissipated by resistance as blood flows through the arterioles, capillaries, and venules. Therefore, the total driving pressure for flow from the peripheral veins to the right atrium is only 10 to 15 mmHg on average. Thus, a major function of the veins is to act as low-resistance conduits for blood flow from the tissues to the heart. The peripheral veins of the arms and legs contain valves that permit flow only toward the heart. In addition to their function as low-resistance conduits, the veins perform a second important function: Their diameters are reflexively altered in response to changes in blood volume, thereby maintaining peripheral venous pressure and venous return to the heart. In a previous section, we emphasized that the rate of venous return to the heart is a major determinant of end-diastolic ventricular volume and thereby stroke volume. We now see that peripheral venous pressure is an important determinant of stroke volume. Determinants of Venous Pressure the factors determining pressure in any elastic tube are the volume of fluid within it and the compliance of its walls. Consequently, total blood volume is one important determinant of venous pressure because, as we will see, most blood is in the veins. Thus, veins can accommodate large volumes of blood with a relatively small increase in internal pressure. During muscle contraction, venous diameter decreases and venous pressure increases. The increase in pressure forces the flow only toward the heart because backward pressure forces the valves in the veins to close. Increased venous pressure then drives more blood out of the veins into the right side of the heart. Note the different effect of venous constriction compared to that of arterioles; when arterioles constrict, the constriction reduces forward flow through the systemic circuit, whereas constriction of veins increases forward flow. Although sympathetic neurons are the most important input, venous smooth muscle, like arteriolar smooth muscle, also responds to hormonal and paracrine vasodilators and vasoconstrictors. Two other mechanisms, in addition to contraction of venous smooth muscle, can increase venous pressure and facilitate venous return. During skeletal muscle contraction, the veins running through the muscle are partially compressed, which reduces their diameter and forces more blood back to the heart. As Chapter 13 describes, at the base of the chest cavity (thorax) is a large muscle called the diaphragm, which separates the thorax from the abdomen. During inspiration of air, the diaphragm descends, pushing on the abdominal contents and increasing abdominal pressure. Simultaneously, the pressure in the thorax decreases, thereby decreasing the pressure in the intrathoracic veins and right atrium. The net effect of the pressure changes in the abdomen and thorax is to increase the pressure difference between the peripheral veins and the heart. Thus, venous return is enhanced during inspiration (expiration would reverse this effect if not for the venous valves), and breathing deeply and frequently, as in exercise, helps blood flow toward the heart. You might get the incorrect impression from these descriptions that venous return and cardiac output are independent entities. Rather, any change in venous return almost immediately causes equivalent changes in cardiac output, largely through the FrankStarling mechanism. Venous return and cardiac output therefore must be the same except for transient changes over brief periods of time. The effects of increased inspiration on end-diastolic ventricular volume are actually quite complex, but for the sake of simplicity, they are shown here only as increasing venous pressure. The lymphatic capillaries are the first of the lymphatic vessels, for unlike the blood vessel capillaries, no tubes flow into them. Small amounts of interstitial fluid continuously enter the lymphatic capillaries by bulk flow. This lymph fluid flows from the lymphatic capillaries into the next set of lymphatic vessels, which converge to form larger and larger lymphatic vessels. Ultimately, the entire network ends in two large lymphatic ducts that drain into the veins near the junction of the jugular and subclavian veins in the upper chest. Valves at these junctions permit only one-way flow from lymphatic ducts into the veins. Thus, the lymphatic vessels carry interstitial fluid to the cardiovascular system. The movement of interstitial fluid from the lymphatics to the cardiovascular system is very important because, as noted earlier, the amount of fluid filtered out of all the blood vessel capillaries (except those in the kidneys) exceeds that absorbed by approximately 4 L each day. In the process, small amounts of protein that may leak out of blood vessel capillaries into the interstitial fluid are also returned to the cardiovascular system. Under some circumstances, the lymphatic system can become occluded, which allows the accumulation of excessive interstitial fluid. Surgical removal of lymph nodes and vessels during the treatment of breast cancer can similarly allow interstitial fluid to pool in affected tissues. In addition to draining excess interstitial fluid, the lymphatic system provides the pathway by which fat absorbed from the gastrointestinal tract reaches the blood (see Chapter 15). The lymphatics can also be the route by which cancer cells spread from their area of origin to other parts of the body (which is why cancer treatment sometimes includes the removal of lymph nodes). Present in the interstitium of virtually all organs and tissues are numerous lymphatic capillaries that are completely distinct from blood vessel capillaries. Like the latter, they are tubes made of only a single layer of endothelial cells resting on a basement membrane, but they have large water-filled channels that are permeable to all interstitial fluid constituents, 404 Chapter 12 In large part, the lymphatic vessels beyond the lymphatic capillaries propel the lymph within them by their own contractions. The smooth muscle in the wall of the lymphatics exerts a pumplike action by inherent rhythmic contractions. Because the lymphatic vessels have valves similar to those in veins, these contractions produce a one-way flow toward the point at which the lymphatics enter the circulatory system. The lymphatic vessel smooth muscle is responsive to stretch, so when no interstitial fluid accumulates and, therefore, no lymph enters the lymphatics, the smooth muscle is inactive. However, when increased fluid filtration out of capillaries occurs, the increased fluid entering the lymphatics stretches the walls and triggers rhythmic contractions of the smooth muscle. This constitutes a negative feedback mechanism for adjusting the rate of lymph flow to the rate of lymph formation and thereby preventing edema. In addition, the smooth muscle of the lymphatic vessels is innervated by sympathetic neurons, and excitation of these neurons in various physiological states such as exercise may contribute to increased lymph f low. These include the same external forces we described for veins - the skeletal muscle pump and respiratory pump. The arteries function as low-resistance conduits and as pressure reservoirs for maintaining blood flow to the tissues during ventricular relaxation. The difference between maximal arterial pressure (systolic pressure) and minimal arterial pressure (diastolic pressure) during a cardiac cycle is the pulse pressure. Mean arterial pressure can be estimated as diastolic pressure plus one-third of the pulse pressure. Arterioles are the dominant site of resistance to flow in the vascular system and play major roles in determining mean arterial pressure and in distributing flows to the various organs and tissues.
For the great majority of antigens antibiotic justification form order cheap zithromax on-line, however antimicrobial 2012 cheap 100 mg zithromax otc, antigen binding is not enough antibiotic names medicine zithromax 500mg on line, and signals in the form of cytokines released into the interstitial fluid by helper T cells near the antigen-bound B cells are also required antibiotic eye drops for conjunctivitis zithromax 100mg mastercard. A helper T cell specific for the complex then binds to it virus que esta en santo domingo purchase discount zithromax, beginning the activation of the helper T cell antibiotics quiz questions purchase 100 mg zithromax otc. Once activated, helper T cells migrate to lymph nodes where they interact with antigen-presenting B cells. The helper T cell stimulates B-cell activation by direct contact and cytokine release. Once activated, the B cell differentiates into a plasma cell that secretes antibodies that recognize the specific antigen. In secondary lymphoid organs, bacterial antigen binds to specific receptors on the plasma membranes of B cells. These activate antigen-bound B cells to proliferate and differentiate into plasma cells. The plasma cells secrete antibodies specific for the antigen that initiated the response, and the antibodies circulate all over the body via the blood. These antibodies combine with antigen on the surface of the bacteria anywhere in the body. Presence of antibody bound to antigen facilitates phagocytosis of the bacteria by neutrophils and macrophages. It also activates the complement system, which further enhances phagocytosis and can directly kill the bacteria by the membrane attack complex. The secreted antibodies travel by the blood to the site of infection, where they bind to bacteria of the type that induced the response. The binding of the helper T cell to the antigen-bound B cell ensures maximal stimulation of the B cell by the cytokines secreted by that helper T cell and any of its progeny that remain nearby. Antibody Secretion After their differentiation from B cells, plasma cells produce thousands of antibody molecules per second before they die in a day or so. The most abundant are the IgG antibodies, commonly called gamma globulin, and IgM antibodies. These two groups together provide the bulk of specific immunity against bacteria and viruses in the extracellular fluid. IgE antibodies participate in defenses against 672 Chapter 18 multicellular parasites and also mediate allergic responses. IgA antibodies are secreted by plasma cells in the linings of the gastrointestinal, respiratory, and genitourinary tracts; these antibodies generally act locally in the linings or on their surfaces. They are also secreted by the mammary glands and, therefore, are the major antibodies in milk. In the kind of infection described in this chapter, the B cells and plasma cells, sitting on the nodes near the infected tissues, recognize antigen and are activated to make antibodies. The antibodies (mostly IgG and IgM) circulate through the lymph and blood to return to the infected site. These antibodies then direct the attack (see following discussion) against the bacteria to which they are now bound. Consequently, immunoglobulins play two distinct roles in immune responses during the initial recognition step: (1) Those on the surface of B cells bind to antigen brought to them; and (2) those secreted by the plasma cells (antibodies) bind to bacteria bearing the same antigens, "marking" them as the targets to be attacked. This linkage not only triggers the attack mechanism but ensures that the killing effects are restricted to the microbe. Linkage to specific antibodies helps protect adjacent normal structures from the toxic effects of the chemicals employed by the killing mechanisms. This linkage promotes attachment of the antigen to the phagocyte and the triggering of phagocytosis of the bacterium. Activation of the Complement System As described earlier in this chapter, the plasma complement system is activated in nonspecific (innate) inflammatory responses via the alternative complement pathway. In contrast, in adaptive immune responses, the presence of antibody of the IgG or IgM class bound to antigen activates the classical complement pathway. This results in activation of the enzymatic portions of C1, thereby initiating the entire classical pathway. Because the latter are the same in virtually all antibodies of the IgG and IgM classes, the complement molecule will bind to any antigenbound antibodies belonging to these classes. In other words, there is only one set of complement molecules and, once activated, they do essentially the same thing regardless of the specific identity of the invader. Antibody-Dependent Cellular Cytotoxicity We have seen that both a particular complement molecule (C1) and a phagocyte can bind nonspecifically to the Fc portion of an antibody bound to antigen. Direct Neutralization of Bacterial Toxins and Viruses Toxins secreted by bacteria into the extracellular fluid can act as antigens to induce antibody production. The antibodies then combine with the free toxins, thereby preventing interaction of the toxins with susceptible cells. Because each antibody has two binding sites for antigen, clumplike chains of antibodyantigen complexes form, and these clumps are then phagocytosed. Activation of classical complement pathway by binding of antibody to bacterial antigen. The Immune System 673 A similar binding process occurs as part of the major antibody-mediated mechanism for eliminating viruses in the extracellular fluid. Certain of the viral surface proteins serve as antigens, and the antibodies produced against them combine with them, preventing attachment of the virus to plasma membranes of potential host cells. As with bacterial toxins, chains of antibodyvirus complexes are formed and can be phagocytosed. Active and Passive Humoral Immunity the response of the antibody-producing machinery to invasion by a foreign antigen varies enormously, depending upon whether the machinery has previously been exposed to that antigen. This response, which is mediated by the memory B cells described earlier, is one of the key features that distinguishes innate and adaptive immunity. It confers a greatly enhanced resistance toward subsequent infection with that particular microorganism. Until the twentieth century, the only way to develop active immunity was to suffer an infection, but now the injection of microbial derivatives in vaccines is used. A vaccine may consist of small quantities of living or dead pathogens, small quantities of toxins, or harmless antigenic molecules derived from the microorganism or its toxin. The general principle is always the same: Exposure of the body to the antigenic substance results in an active immune response along with the induction of the memory cells required for rapid, effective response to possible future infection by that particular organism. A second kind of immunity, known as passive immunity, is simply the direct transfer of antibodies from one person to another, the recipient thereby receiving preformed antibodies. Such transfers occur between mother and fetus because IgG can Amount of specific antibody in plasma (arbitrary units) move across the placenta. These are important sources of protection for the infant during the first months of life, when the antibody-synthesizing capacity is relatively poor. The same principle is used clinically when specific antibodies (produced by genetic engineering) or pooled gamma globulin injections are given to patients exposed to or suffering from certain infections such as hepatitis. Because antibodies are proteins with a limited life span, the protection afforded by this transfer of antibodies is relatively short-lived, usually lasting only a few weeks or months. Summary It is now possible to summarize the interplay between innate and adaptive immune responses in resisting a bacterial infection. When a particular bacterium is encountered for the first time, innate defense mechanisms resist its entry and, if entry is gained, attempt to eliminate it by phagocytosis and nonphagocytic killing in the inflammatory process. Simultaneously, bacterial antigens induce the relevant specific B-cell clones to differentiate into plasma cells capable of antibody production. If the innate defenses are rapidly successful, these slowly developing specific immune responses may never play an important role. If the innate responses are only partly successful, the infection may persist long enough for significant amounts of antibody to be produced. The presence of antibody leads to both enhanced phagocytosis and direct destruction of the foreign cells, as well as to neutralization of any toxins the bacteria secrete. All subsequent encounters with that type of bacterium will activate the specific responses much sooner and with greater intensity. The defenses against viruses in the extracellular fluid are similar, resulting in destruction or neutralization of the virus. Defenses Against Virus-Infected Cells and Cancer Cells the previous section described how antibody-mediated immune responses constitute the major long-term defense against exogenous antigens - bacteria, viruses, and individual foreign molecules that enter the body and are encountered by the immune system in the extracellular fluid. Such destruction results in release of the viruses into the extracellular fluid, where they can be directly neutralized by circulating antibody, as just described. The sequence would be similar if the inducing cell were a cancer cell rather than a virus-infected cell. Cytotoxic T cells specific for the particular antigen can bind to the complex; just as with B cells, however, binding to antigen alone does not cause activation of the cytotoxic T cell. Other cytokines secreted by the activated helper T cell perform the same functions. Why is proliferation important if a cytotoxic T cell has already found and bound to its target? The answer is that there is rarely just one virus-infected cell or one cancer cell. By expanding the clone of cytotoxic T cells capable of recognizing the particular antigen, proliferating attack cells increase the likelihood that other virus-infected or cancer cells will be encountered by the specific type of cytotoxic T cell. The cytotoxic T cell releases, by exocytosis, the contents of its secretory vesicles into the extracellular space between itself and the target cell to which it is bound. However, it is believed that at least one mechanism by which perforin acts is to facilitate the transport of cytotoxic enzymes called granzymes, released by the cytotoxic T cells, into the infected cell. These enzymes then activate intracellular enzymes that induce apoptosis, killing the cell. The fact that perforin is released directly into the space between the tightly attached cytotoxic T cell and the target ensures that uninfected host bystander cells will not be killed, because perforin is not at all specific. The Immune System 675 Some cytotoxic T cells generated during proliferation following an initial antigenic stimulation do not complete their full activation at this time but remain as memory cells. In addition to phagocytosis, they secrete large amounts of many chemicals that are capable of killing cells by a variety of mechanisms. As long as there is a pathogen at the site of infection, activated macrophages will continue to present antigens to T cells that will maintain the ensuing immune response. Once cleared of infection, tissue repair will continue and the immune response will wane as T cells are no longer being activated against the pathogen. The single most common and striking systemic sign of infection is fever, the mechanism of which is described in Chapter 16. Present evidence suggests that moderate fever can be beneficial because an increase in body temperature enhances many of the protective responses described in this chapter. Decreases in the plasma concentrations of iron and zinc occur in response to infection and are due to changes in the uptake and/or release of these elements by liver, spleen, and other tissues. The decrease in plasma iron concentration has adaptive value because bacteria require a high concentration of iron to multiply. Another adaptive response to infection is the secretion by the liver of a group of proteins known collectively as acute phase proteins. These proteins exert many effects on the inflammatory process that serve to minimize the extent of local tissue damage. In addition, they are important for tissue repair and for clearance of cell debris and the toxins released from microbes. An example of an acute phase protein is C-reactive protein, which functions as a nonspecific opsonin to enhance phagocytosis. Another response to infection, increased production and release of neutrophils and monocytes by the bone marrow, is of obvious value. Also occurring is a release of amino acids from muscle; the amino acids provide the building blocks for the 18. The effect of cortisol on the immune response is inhibitory; cortisol provides a negative feedback action to prevent excessive immune activity (see Chapter 11 for the control mechanisms and basic functions of cortisol). The Immune System 677 synthesis of proteins required to fight the infection and for tissue repair. Increased release of fatty acids from adipose tissue also occurs, providing a source of energy. The secretion of many hormones - notably, cortisol - is increased in the acute phase response, exerting negative feedback actions on immune function. Several other cytokines are also known to participate in the acute phase response. For example, colony-stimulating factors, which are secreted by macrophages, lymphocytes, endothelial cells, and fibroblasts, provide a major stimulus to the bone marrow to produce more neutrophils and monocytes. The participation of macrophages in the acute phase response completes our discussion of these cells, the various functions of which are summarized in Table 18. Proteincalorie malnutrition is, worldwide, the single greatest contributor to decreased resistance to infection. Because inadequate amino acids are available to synthesize essential proteins, immune function is impaired. Deficits of specific nutrients other than protein can also lower resistance to infection. A preexisting disease, infectious or noninfectious, can also predispose the body to infection. People with diabetes mellitus, for example, are more likely to develop infections, at least partially explainable on the basis of defective leukocyte function. They also secrete antimicrobial chemicals and protein messengers (cytokines) that function as local inflammatory mediators. There are multiple mechanisms that constitute the links in these "mindbody" interactions.

















